
1. Failures, Reoperations, Complications
There is no large single-surgeon report of THR or HRA that can match the results reported here. Most failures occur during the first year after surgery, which is why it is critical to severely limit activities in the first 6 months to allow adequate healing. After that, a patient can gradually return to completely unrestricted activity. There remains a slow rate of failure that occurs over time. But this does not seem to be affected by activity. Therefore, the overall failure rate increases for a group of patients as the length of follow-up increases. In this section we report all complications that we know of for the Uncemented Recap/Magnum system from 2007-2022. This means all patients are at least 4 years postop. This group is comprises 5375 cases. I currently have performed over 6500 of these implants. It is challenging, but I am typically able to maintain a greater than 90% rate of up-to-date follow-up on my patients. Failures are those complications that have led to revision surgery (one or both implants have been replaced), Reoperation means a second operation has been required to correct a problem, but the original implants are retained. Other complications are ones in which no further surgery has been performed. I also use other resurfacing implants but only have long-term data available on two of them (Corin Cormet 2000, and Hybrid Recap/Magnum, Smith Nephew BHR, Joint Medica Polymotion).
I. Failures (At least one implant replaced)
| Type | #, % |
|---|---|
| # Cases | 5375 |
| 1) Acetabular Failures | |
| Adverse Wear | 6 (0.1%) |
| Acetabular Loosening (>2 years) | 11 (0.2%) |
| Failure of Acetabular Ingrowth (<2 years) | 11 (0.2%) |
| Acetabular Component Shift1 | 6 (0.1%) |
| 2) Femoral Failures | |
| Early Femoral Head Collapse (<6 months) | 4 (0.07%) |
| Femoral Component Loosening | 3 (0.06%) |
| Early Femoral Fracture (<6 months) | 17 (0.3%) |
| 3) Other Failures | |
| Recurrent Instability | 8 (0.1%) |
| Early Infection (<1 year) | 0 (0.0%) |
| Late Infection (>1 year) | 3 (0.06%) |
| Late Fracture | 20 (0.4%) |
| Unexplained Pain | 5 (0.1%) |
| Psoas Tendonitis | 3 (0.06%) |
| Other | 7 (0.1%) |
| TOTAL FAILURES | 104 (1.9%) |
1 Did not begin capturing Acetabular Component Shifts until Dec 2007.
II. Reoperations (no implants revised)
| Type | #, % |
|---|---|
| # Cases | 5375 |
| Acetabular Component Shift | 1 (<0.1%) |
| Gluteal Tear | 1 (<0.1%) |
| Dislocation | 1 (<0.1%) |
| Early Fracture (<6 months) | 2 (<0.1%) |
| Early Infection (<3 months) | 4 (0.1%) |
| Early Infection (<1 year) | 6 (0.1%) |
| Late Infection (>1 year) | 0 (0.0%) |
| Fascia Failure | 3 (0.1%) |
| Hematoma | 4 (0.1%) |
| Late Fracture (>6 months) | 13 (0.2%) |
| Psoas Tendonitis | 1 (<0.1%) |
| Unexplained Swelling | 2 (<0.1%) |
| Other | 3 (0.1%) |
| TOTAL REOPERATIONS | 37 (0.7%) |
III. Complications (no additional surgery required)
| Type | #, % |
|---|---|
| # Cases | 5375 |
| Acetabular Component Shift | 30 (0.6%) |
| Dislocation | 22 (0.4%) |
| Anxiety | 3 (0.1%) |
| Early Fracture (<6 months) | 5 (0.1%) |
| Late Fracture (>6 months) | 6 (0.1%) |
| Early Infection (<3 months) | 1 (<0.1%) |
| Fascia Failure | 1 (<0.1%) |
| Femoral Component Shift | 4 (0.1%) |
| Hematoma | 5 (0.1%) |
| PE/DVT | 16 (0.3%) |
| Nerve Palsy | 7 (0.1%) |
| Spinal Headache | 7 (0.1%) |
| Severe Constipation | 2 (<0.1%) |
| Urinary Retention | 8 (0.1%) |
| GI Bleed | 2 (<0.1%) |
| Unexplained Swelling/Pain | 3 (<0.1%) |
| Nausea/Vomiting | 2 (<0.1%) |
| Other | 7 (0.2%) |
| TOTAL COMPLICATIONS | 132 (2.5%) |
IV. Unexplained pain and dissatisfaction
Unexplained pain means that a patient has significant residual pain that we cannot discover the cause for. I will follow a patient for 1-2 years and perform multiple tests to try to discover the source of residual pain. Sometimes they just turn the corner after 6 months -1 year and get better. Sometimes there may be referred pain from their back or there may be soft tissue problems around the hip which we are unable to diagnose. Even MRI cannot find the source of the problem in many cases. In a THR thigh pain from the stem is a common cause of residual pain, this is not correctable; this does not occur with HRA. Residual pain may just represent the fact that HRA does not result in a normal hip. Sometimes the problem was “poor patient selection”. For example, patients who have a lot of pain but have only minor X-ray abnormalities are more likely to end up with residual unexplained pain and be dissatisfied. Unfortunately, sometimes THR surgeons who have little experience with HRA “diagnose” a cause in a painful HRA and perform a revision to a THR. In over 50% of these cases the patient does not get better and we can only presume that the THR surgeon was incorrect in his diagnosis. I will not offer revision surgery to patients who have had their original HRA or THR elsewhere if I cannot discover a source of pain with their implant. In patients in which I have done the original surgery, I will revise them to a THR after 2 years even if no cause can be determined if they insist, but the success rate for this undertaking is low and I recommend against it.
Among unrevised cases, the satisfaction rate was 98.1% . Another 38 patients did not follow-up or expressed not wanting to follow-up. Assuming all were dissatisfied yields a worst-case dissatisfaction rate of 2.6%. The rate of revision for unexplained pain was 0.1%. Among the unrevised cases, the rate of patient-reported residual moderate or greater pain was 0.9% at latest follow-up. Of these, the rate of known significant concomitant lumbar spine disease was 57.4%. The dissatisfaction rate for THR is 10% while the rate of moderate to severe residual pain is 20%.
We cannot cure hip pain 100% of the time even with a perfectly executed operation. But the odds of achieving an excellent outcome are far greater with HRA than THR.
2. Implant Survivorship
Includes all implant types*: 7000 cases over 20 years
*unless noted otherwise in each graph
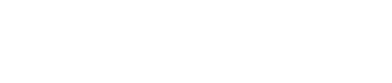
Implant Survivorship is a measure of how long your operation is likely to last. All operations have a failure rate that gradually increases over time. Comparing Kaplan-Meier (KM) survivorship between surgeons and different types of operations allows you to understand likely durability. Unfortunately this type of data is very hard to get for most surgeons or operations.
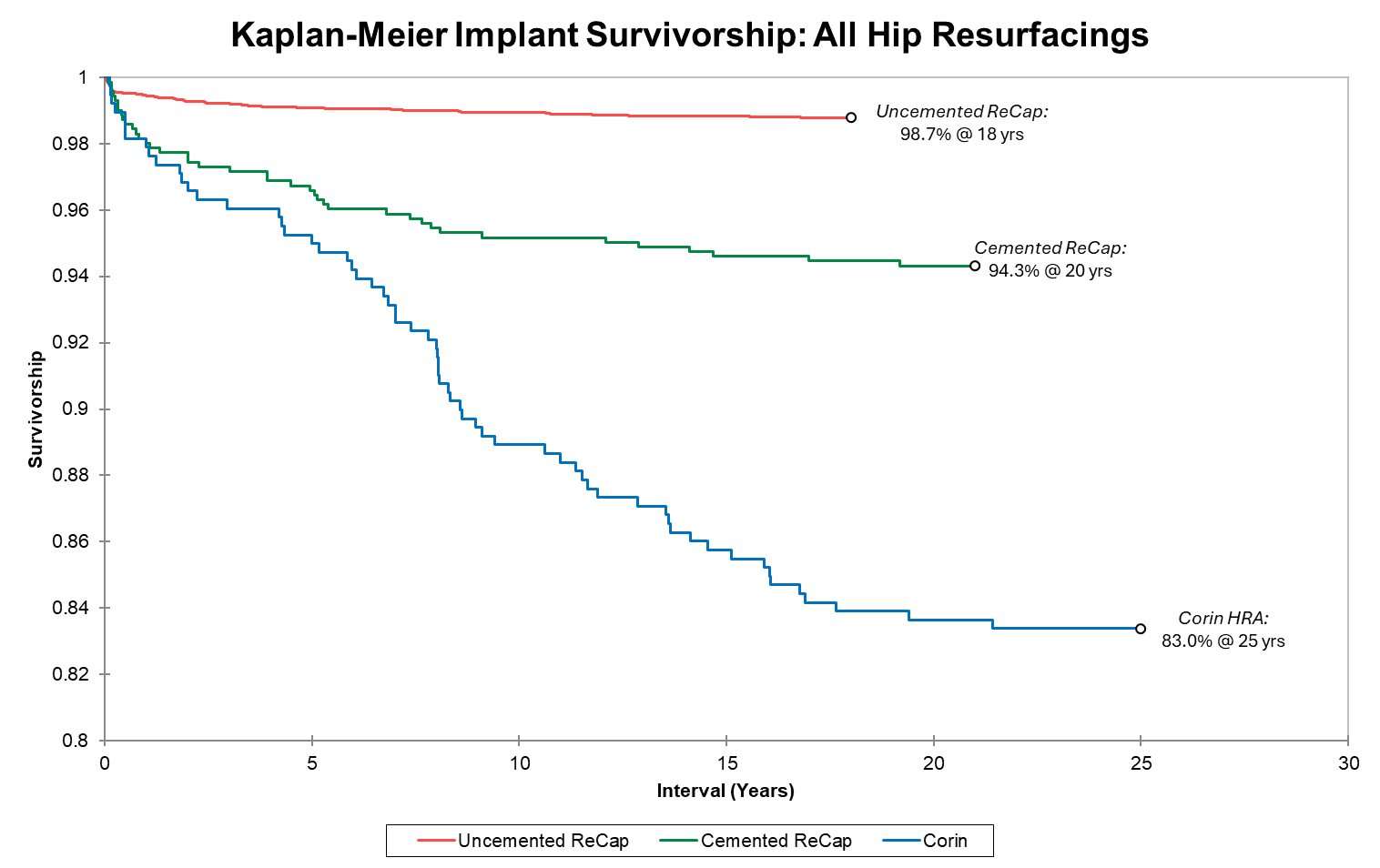
Survivorship of hip resurfacing continues to improve as we gain more experience and identify measures to prevent failures. We present three KM survivorship curves: all implant groups, all implants for patients under 50 at time of surgery, and Recap/Magnum implants grouped by sex. Unlike for THR, HRA survivorship does not vary by age (overall 99.1% 16-year implant for both age groups) Most failures occur in the first 1-2 years. If you make it to one year, your implant survivorship at 13 years is 99.6%. If you make it to 2 years, it is 99.8%. Dr. Gross' uncemented resurfacing implant survivorship beats all international registry benchmarks for THR regardless of age or sex. In our recent multicenter international study (27 HRA centers in 13 countries), over 11,000 cases in patients under age 50 with multiple different metal-on-metal HRA brands showed a 90% 20-year implant survivorship (93% in men and 81% in women). For comparison, THA registries show approximately 80% implant survivorship at 10 years and 50% at 20 years in this age group.
Note that the survivorship y-axis begins at 80%. There have been no instances of adverse metal wear from any surgeries performed after 2009. Long-term implant survivorship continues to improve. Our first resurfacing group was 373 Corin cases beginning in 2002. At 25 years, this group’s implant survivorship exceeds registry data for THR in young patients. As our knowledge, skill, and implant quality improved, so did results. We began our next Recap hybrid implant (n=750) in 2005; with >94% implant survivorship at 20 years, this far exceeds THR registry data. Lastly, we began using the Recap uncemented implants in 2007 (n>6200); survivorship for this group at 18 years is 98.7%.
Above is the survivorship curve separate by age group for our uncemented ReCap group. Note the y-axis start at 90%. There is no difference in survivorship or raw failure rate based on age.
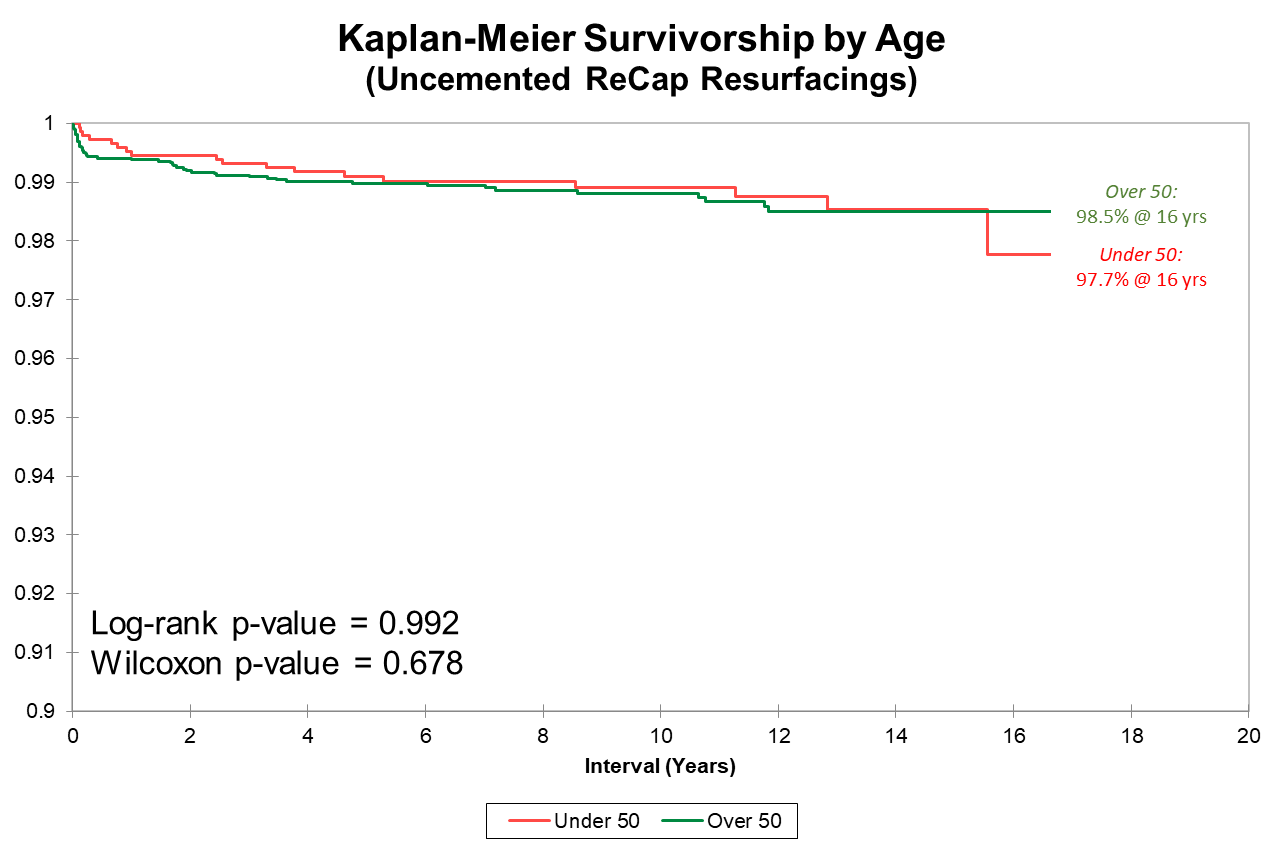
Many orthopedic surgeons exclude women from HRA because of poor published results. We, however, elected to investigate why implants in women were underperforming and to adjust implant design + surgical technique rather than exclude women from surgery. After implementation of new protocols from 2007-2009, implant survivorship between men and women is not significantly different.
The implant survivorship data reported here far surpasses joint implant registry data from Britain, Sweden and Australia (for both THR and HRA) where these types of data are kept. These are publicly available, and you can get access them online for free. Registry data can be thought of as average surgeon implant survivorship for purposes of a benchmark. But the most important factor in the outcome of any operation is individual surgeon skill. It is hard to know at which level a surgeon you are considering can perform. Anecdotal reports from a few patients or reputation are a poor substitute for data. Few surgeons provide written data such as I do.
Remember, implant survivorship is not the only factor that needs to be considered in deciding between THR and HRA. Other proven advantages of HRA include better functional outcome, less residual thigh pain, fewer short and long-term fractures, fewer dislocations, fewer wear/corrosion failures, bone preservation, and longer life expectancy of the patient (lower 10-year all-cause mortality)
Past results do not guarantee future complication rates. Although the above represent the most common complications associated with this procedure, others could also occur. We continue to strive to make improvements, and hope that these complication rates can be further decreased as we gain even more experience.
Current implants that Dr. Gross uses include the metal-on-metal uncemented Biomet Recap/Magnum, the metal-on-metal hybrid Smith Nephew Birmingham Hip Resurfacing, and the hybrid metal-on-polyethylene Joint Medica Polymotion Hip Resurfacing. Please discuss details of implant type and your preferences with Dr. Gross.