
Updated on 27th March 2026
Mission Statement
I am a specialist in the field of hip and knee replacement. I am in private practice but involved in clinical research, teaching, and orthopedic implant development. I perform all my surgeries personally, with the assistance of Lee Webb, DNP. No residents or fellows conduct your operation. Visiting surgeons are occasionally present to observe my operations but do not participate in the operations themselves. I have received royalties and research support from various orthopedic implant companies. I am not paid for the hardware used in your surgery - implants in the Columbia marketplace are excluded from my royalty contracts. I will answer any specific questions you have regarding implants to be used in your operation.
It is the standard of care for joint replacement surgeons to provide long-term follow-up evaluations for their patients. Although we do bill for these services, we primarily earn our living from surgery. As a surgeon involved in clinical research, it is particularly important to me to continue a long-term relationship with all patients on whom I operate. I use data gathered in my practice as material for informing patients, improving my outcomes, teaching, scientific presentations, and clinical papers. Patient identity is carefully protected in all mediums. (The only exception is for patients who specifically agree to publicly share a personal testimonials/description of their case.) You benefit from the improvements in outcomes that have been driven by past clinical research and we ask you to pay this forward for future patients by continuing to follow-up with me. Also, if we maintain accurate records on your case, we have something to compare to when you call with a problem several years later. This helps us better understand any new problem with your hip and helps us solve it.
Every medical/surgical treatment has potential for complications. I disclose these to you in the consent form provided; a regularly updated list of complications among my patient cohort are posted to my website. If you should have a complication, I will deal with it promptly and directly. Even out of state patients should keep me well informed of any that develop. It is my preference (and in your best interest) for me to deal with all surgical complications personally. Nonsurgical (medical) complications can be dealt with by your local primary care physician or other non-orthopedic specialist, but please keep me informed/allow me to advise you. Surgical complications may require unexpected trips to Columbia, SC. Many patients have chosen me as their surgeon due to my low rates of complications/revisions. However, equally important is my knowledge in how to deal with postoperative complications. Even after they occur, a good outcome can often be achieved with appropriate, skilled intervention.
I expect to see all patients for follow up evaluations at four- to six- weeks postoperatively and one-year postoperatively. If you are an out of state patient, remote follow up can be arranged (but is not preferred). If your case is routine and stable, long-term follow up (>2 years postoperative) can be done via online questionnaire and digital x-ray. I will provide you with a written reply and will not charge you for reviewing your materials. If a phone consultation is required (after three months post-op) a fee may be assessed. If you do have specific problems that can’t be solved by advice given over the telephone, on-site evaluation by me is recommended. My commitment to you is the highest level of care, both technically and personally. I strive to continue to elevate the level of my expertise by dealing with complications directly and promptly, and by continuing a rigorous and systematic scientific review of my surgical outcomes.
Expectations after Hip Resurfacing Surgery
Hip resurfacing arthroplasty (HRA) is an operation that is used to treat severe hip arthritis and is offered by me as an alternative to the standard operation of stemmed total hip replacement (THR).
Most surgeons in the world will recommend a standard stemmed THR to treat your condition. Although this is an excellent operation and is generally quite successful, I believe that I can do better job for you with an HRA. If you would prefer a standard stemmed THR, I would tell you that your chances of an excellent outcome are better with an HRA, but the choice is yours to make. I would do either operation for you. I have published excellent long-term outcomes with both operations that substantially outperform industry benchmarks (Registry data).
The material risks of HRA are spelled out in great detail in both the consent form as well as on my website that I have encouraged you to review.
No one is able to make your hip completely normal. But I am likely to get much closer to this goal if I perform a HRA rather than a THR. Outright failures leading to revision (changing out implants) surgery occur in approximately 1% of cases before 1 year and less than 3% at 18 years. Reoperations (corrective operations where the implants are not removed) are required in less than 1%. Other complications not requiring another operation occur in another 2%. This is the highest published success rate for any type of hip surgery in North America.
Immediately after surgery your original hip pain caused by missing cartilage is gone. This is because I have prepared the bone and fixed an implant into the bone on both sides of the joint. Painful bone rubbing on bone has been converted to painless implant rubbing on implant. Postoperative pain is mainly a result of the controlled surgical trauma required to get access to your hip. Initially surgical pain is much worse than your original arthritic pain. This is why we use a multimodal pain management system including some narcotics to keep you reasonably comfortable. However, many (not all) people can qualitatively tell the difference between their old arthritic pain and the new muscle pain. It may feel much like a severe bruise. The soft tissue pain rapidly subsides within a few days. Most people stop using narcotics after 3-4 days and discontinue Tylenol, meloxicam and ice after 2 weeks.
Patients are usually able to resume walking and dispense with walking aids within a few weeks. But we need to limit activity to some extend for 6 months to allow adequate healing. People with very low bone density or a BMI>30 are at higher fracture risk and are advised to stay on crutches for 6 weeks to mitigate this risk.
The implant needs to achieve bone ingrowth, the ligaments and muscle need to heal and the bone is fragile for about 6 months. Excessive activity is damaging to the healing process The most common early failure mode is femoral neck fracture. This requires revision to a stemmed THR. These always occur in the first 6 months. The overall incidence is 0.2% (1/500). Patients who have low bone density and those with a BMI of over 29 are at higher risk. To mitigate risk in these groups, we prescribe bone strengthening medication and a slow (10 -week) restricted weight bearing protocol. With these measures the risk in these high-risk groups is similar to the other patients. These fractures are typically stress fractures that happen spontaneously or from minor falls that don’t normally result in a serious injury.
Most operations are performed as outpatient procedures in the ambulatory surgery center (ASC) that is owned by my group. The approach is posterior. The typical surgical time is 1.5 hours, the mean blood loss is 200 ml and you will not require a transfusion . After surgery you walk around the center and climb stairs with the nurse or therapist. You are given all your required medication. We give your caregiver detailed instructions and a written 6 page handout that records these for you in great detail. When you are eating, drinking urinating and walking with assistance you are released. Usually in under 3 hours after coming out of surgery. Your pain will be well-controlled with a multimodal pain management protocol. You will be given contact phone numbers to reach us anytime you need us.
In the typical recovery patients are able to
- Drive in 3-4 days as soon as they are off narcotics (using the left foot on the brake for right -sided surgery).
- Return to a desk job within 1-2 weeks.
- Resume upper extremity workouts without loading the legs in 2 weeks.
- Use crutches ( weight as tolerated ) for 1-2 weeks, and a cane in the opposite hand for 1-2 weeks.
- Progress to walking to one mile by 6 weeks. This should be viewed as maximum ceiling to minimize fracture risk. My motto is “less is more” during the first 6 weeks.
- Initially stairs are ascended one foot at a time, at 6 weeks you can start foot over foot stair climbing with assistance of a rail.
- Return to moderately physical job that requires a lot of walking by 6 weeks.
- Impact sports and heavy labor are allowed at 6 months.
There is reason to believe that fracture risk may be further reduced below 0.2% by just remaining on crutches for the full 6 weeks. You can choose this depending on your risk tolerance. On the other hand, if you do more than I recommend, you are increasing your fracture risk.
For typical patients, at 6 weeks I approve of gradually increasing walking distances beyond 1 mile, gently using an exercise bike or elliptical, swimming, gradually returning to golf, gently starting some lower extremity resistance and weight training up to 50 pounds.
Recommended restrictions up to 6 months are:
- Impact activities such as running and jumping
- Stairclimbing exercises
- Lifting more than 50 pounds.
- Extreme bending such as squats or yoga.
- Fall risk activities such as ladder climbing or biking outside.
At 6 months the fracture risk has essentially resolved, the implant is well ingrown and the ligaments are healed. You are released to unrestricted activity including heavy labor, impact sports and high range of motion activities such as yoga.
The most extreme activities such as unprotected rock climbing, slide tackling in soccer, jumping out of airplanes, sport fighting, and ski jumping should be avoided until 1 year.
Most patients feel better than before surgery at 6 weeks, but some take as long as one year to turn the corner. For most people I would estimate healing to be 90% complete at 6 months, 98% complete at 1 year and 100% at 2 years. Over half of patients after 2 years say their hip feels completely normal. The other half say it is near normal with some minor residual issues. About 2 percent say they have moderate or severe residual pain; 1 percent are not satisfied. For comparison, the rate of residual moderate or greater unexplained pain or dissatisfaction in total knee replacement is 30% and in stemmed total hip replacement is 20%. In patients who are dissatisfied with a THR or HRA done elsewhere, I will only offer revision surgery if I can reasonably determine a cause of failure, I do not perform exploratory revisions for unexplained pain because it carries a less than 50% success rate. On the other hand, if one of my patients has residual unexplained pain after 1 year, I would reluctantly agree to perform a revision to a THR, but I would recommend against it because of the low success rate. Unexplained pain means significant residual pain after surgery for which no obvious cause can be found on detailed testing: X-rays, ions, other bloodwork, MRI and bone scan.
Running is possible for all HRA patients (unless they have another problem that limits it). Almost all patients can run a few miles. Distance running, however, is not always tolerated. It is, however encouraged. Running does not increase your implant failure rate. The cause of distance running tolerance is not understood. I would simply say that I never make anyone a normal hip. For some people a hip resurfacing is not good enough to tolerate this extreme activity. In those that don’t initially tolerate running at 6 months, persistently running multiple times a week up to the point of soreness but not pain can lead to improvement. Running or other extreme impact sports do not seem to affect the failure rate of HRA, they are generally poorly tolerated in patients with stemmed THR and do increase the failure rate of THR implants.
My published cumulative failure rate is approximately 2% by 18 years in a very large cohort of over 6000 cases. This is superior to any THR report from Europe or North America. Failure means that a revision has been performed, usually for an identified cause such as fracture or implant loosening. All causes of failure, reoperation and other complications are listed in the latest results section on my website.
The advantages of hip resurfacing over THR are:
- Better functional outcome especially with Impact sports, but also with rapid walking. (The THR stem can bother people even at low activity levels).
- Preference: 85% of patients who have one of each prefer the resurfacing.
- Fewer dislocations ( Because the ball size is normal in HRA)
- Bone preservation
- Lower short term (0.2 %vs 1-2% by 6 months) and lower long term ( 1% vs 7% by 20 years) fracture rate than for THR.
- Less problems with wear or corrosion. (No wear failures in over 4000 cases since 2009 in my HRA, compared to 1-3 % trunnion corrosion failures with THR)
- Lower 10 year all-cause mortality (20% - 600% in 6 publications)
Disadvantages:
- Technically more demanding to perform with a long learning curve
- Duration of surgery is longer especially for the inexperienced surgeon, increasing the work done for the same CPT code 21730 as stemmed THR.
- Patients with unexplained pain with HRA get unhelpful revisions from THR surgeons. Patients with unexplained pain after THR are not operated on and are left alone.
Failures, Reoperations, Other Complications
There is no large single-surgeon report of THR or HRA that can match the results reported here. Most failures occur during the first year after surgery, which is why it is critical to severely limit activities in the first 6 months to allow adequate healing. After that, a patient can gradually return to completely unrestricted activity. There remains a slow rate of failure that occurs over time. But this does not seem to be affected by activity. Therefore, the overall failure rate increases for a group of patients as the length of follow-up increases. In this section we report all complications that we know of for the Uncemented Recap/Magnum system from 2007-2022. This means all patients are at least 4 years postop. This group is comprises 5375 cases. I currently have performed over 6500 of these implants. It is challenging, but I am typically able to maintain a greater than 90% rate of up-to-date follow-up on my patients. Failures are those complications that have led to revision surgery (one or both implants have been replaced), Reoperation means a second operation has been required to correct a problem, but the original implants are retained. Other complications are ones in which no further surgery has been performed. I also use other resurfacing implants but only have long-term data available on two of them (Corin Cormet 2000, and Hybrid Recap/Magnum, Smith Nephew BHR, Joint Medica Polymotion).
I. Failures (At least one implant replaced)
1 Did not begin capturing Acetabular Component Shifts until Dec 2007.
II. Reoperations (no implants revised)
III. Complications (no additional surgery required)
IV. Unexplained pain and dissatisfaction
Unexplained pain means that a patient has significant residual pain that we cannot discover the cause for. I will follow a patient for 1-2 years and perform multiple tests to try to discover the source of residual pain. Sometimes they just turn the corner after 6 months -1 year and get better. Sometimes there may be referred pain from their back or there may be soft tissue problems around the hip which we are unable to diagnose. Even MRI cannot find the source of the problem in many cases. In a THR thigh pain from the stem is a common cause of residual pain, this is not correctable; this does not occur with HRA. Residual pain may just represent the fact that HRA does not result in a normal hip. Sometimes the problem was “poor patient selection”. For example, patients who have a lot of pain but have only minor X-ray abnormalities are more likely to end up with residual unexplained pain and be dissatisfied. Unfortunately, sometimes THR surgeons who have little experience with HRA “diagnose” a cause in a painful HRA and perform a revision to a THR. In over 50% of these cases the patient does not get better and we can only presume that the THR surgeon was incorrect in his diagnosis. I will not offer revision surgery to patients who have had their original HRA or THR elsewhere if I cannot discover a source of pain with their implant. In patients in which I have done the original surgery, I will revise them to a THR after 2 years even if no cause can be determined if they insist, but the success rate for this undertaking is low and I recommend against it.
Among unrevised cases, the satisfaction rate was 98.1% . Another 38 patients did not follow-up or expressed not wanting to follow-up. Assuming all were dissatisfied yields a worst-case dissatisfaction rate of 2.6%. The rate of revision for unexplained pain was 0.1%. Among the unrevised cases, the rate of patient-reported residual moderate or greater pain was 0.9% at latest follow-up. Of these, the rate of known significant concomitant lumbar spine disease was 57.4%. The dissatisfaction rate for THR is 10% while the rate of moderate to severe residual pain is 20%.
We cannot cure hip pain 100% of the time even with a perfectly executed operation. But the odds of achieving an excellent outcome are far greater with HRA than THR.
Implant Survivorship (Durability)
Includes all implant types*: 7000 cases over 20 years
*unless noted otherwise in each graph
Implant Survivorship is a measure of how long your operation is likely to last. All operations have a failure rate that gradually increases over time. Comparing Kaplan-Meier (KM) survivorship between surgeons and different types of operations allows you to understand likely durability. Unfortunately this type of data is very hard to get for most surgeons or operations.
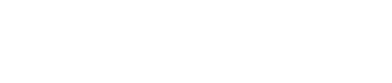
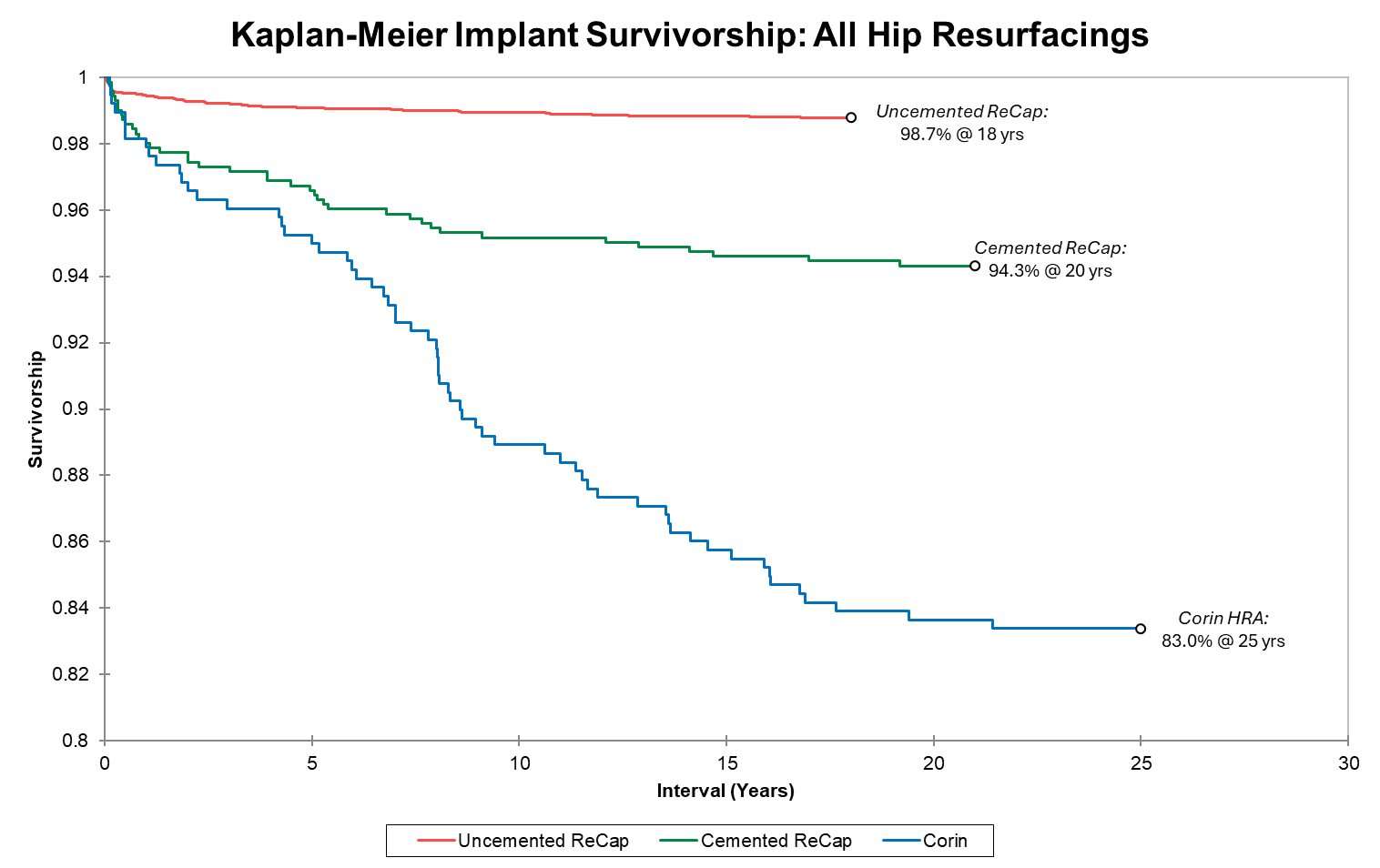
Survivorship of hip resurfacing continues to improve as we gain more experience and identify measures to prevent failures. We present three KM survivorship curves: all implant groups, all implants for patients under 50 at time of surgery, and Recap/Magnum implants grouped by sex. Unlike for THR, HRA survivorship does not vary by age (overall 99.1% 16-year implant for both age groups) Most failures occur in the first 1-2 years. If you make it to one year, your implant survivorship at 13 years is 99.6%. If you make it to 2 years, it is 99.8%. Dr. Gross' uncemented resurfacing implant survivorship beats all international registry benchmarks for THR regardless of age or sex. In our recent multicenter international study (27 HRA centers in 13 countries), over 11,000 cases in patients under age 50 with multiple different metal-on-metal HRA brands showed a 90% 20-year implant survivorship (93% in men and 81% in women). For comparison, THA registries show approximately 80% implant survivorship at 10 years and 50% at 20 years in this age group.
Note that the survivorship y-axis begins at 80%. There have been no instances of adverse metal wear from any surgeries performed after 2009. Long-term implant survivorship continues to improve. Our first resurfacing group was 373 Corin cases beginning in 2002. At 25 years, this group’s implant survivorship exceeds registry data for THR in young patients. As our knowledge, skill, and implant quality improved, so did results. We began our next Recap hybrid implant (n=750) in 2005; with >94% implant survivorship at 20 years, this far exceeds THR registry data. Lastly, we began using the Recap uncemented implants in 2007 (n>6200); survivorship for this group at 18 years is 98.7%.
Above is the survivorship curve separate by age group for our uncemented ReCap group. Note the y-axis start at 90%. There is no difference in survivorship or raw failure rate based on age.
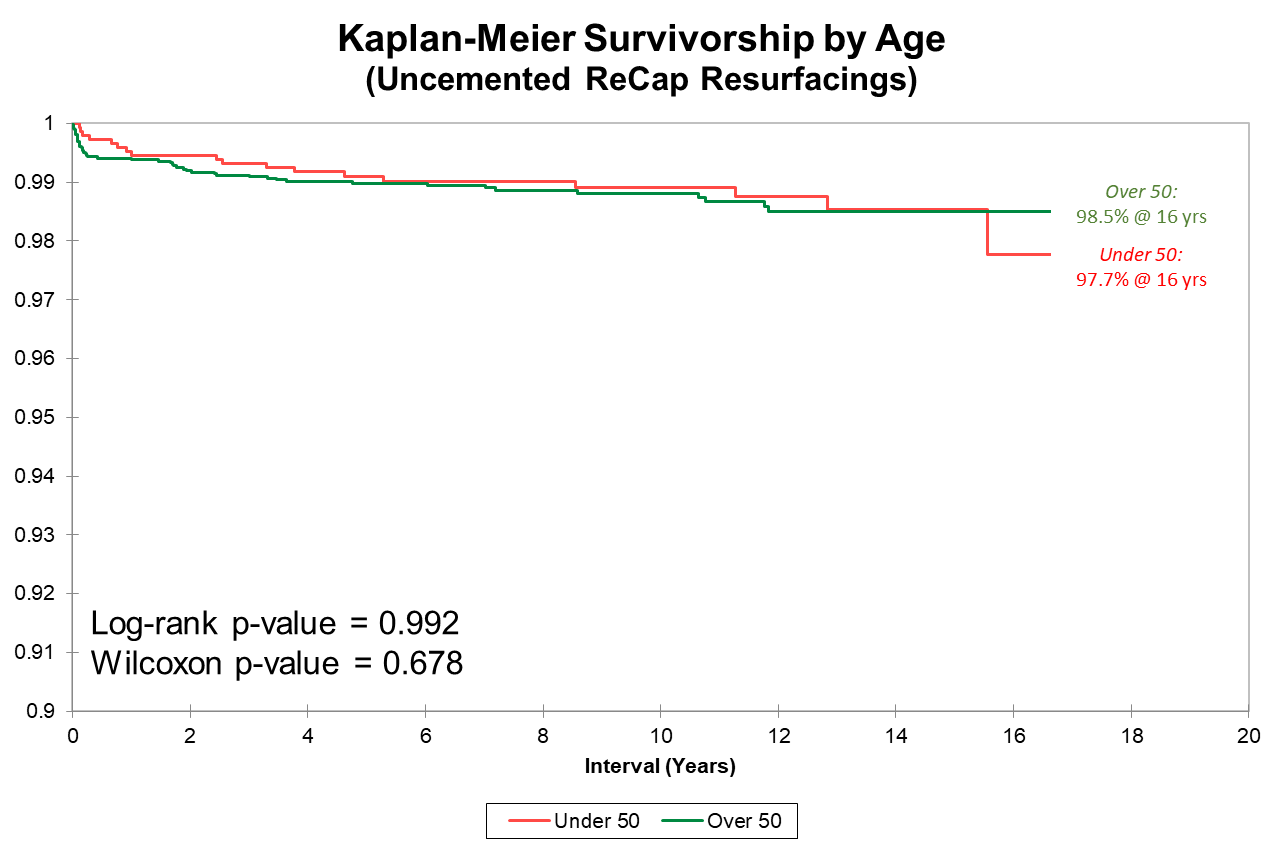
Many orthopedic surgeons exclude women from HRA because of poor published results. We, however, elected to investigate why implants in women were underperforming and to adjust implant design + surgical technique rather than exclude women from surgery. After implementation of new protocols from 2007-2009, implant survivorship between men and women is not significantly different.
The implant survivorship data reported here far surpasses joint implant registry data from Britain, Sweden and Australia (for both THR and HRA) where these types of data are kept. These are publicly available, and you can get access them online for free. Registry data can be thought of as average surgeon implant survivorship for purposes of a benchmark. But the most important factor in the outcome of any operation is individual surgeon skill. It is hard to know at which level a surgeon you are considering can perform. Anecdotal reports from a few patients or reputation are a poor substitute for data. Few surgeons provide written data such as I do.
Remember, implant survivorship is not the only factor that needs to be considered in deciding between THR and HRA. Other proven advantages of HRA include better functional outcome, less residual thigh pain, fewer short and long-term fractures, fewer dislocations, fewer wear/corrosion failures, bone preservation, and longer life expectancy of the patient (lower 10-year all-cause mortality)
Past results do not guarantee future complication rates. Although the above represent the most common complications associated with this procedure, others could also occur. We continue to strive to make improvements, and hope that these complication rates can be further decreased as we gain even more experience.
Current implants that Dr. Gross uses include the metal-on-metal uncemented Biomet Recap/Magnum, the metal-on-metal hybrid Smith Nephew Birmingham Hip Resurfacing, and the hybrid metal-on-polyethylene Joint Medica Polymotion Hip Resurfacing. Please discuss details of implant type and your preferences with Dr. Gross.
Consent
I have read the entire 10 page document above and have been encouraged to and have had ample opportunity to review much more detailed information available about Hip Resurfacing by Dr. Thomas Gross on his website grossortho.com. All of my questions about this document and about my operation have been answered to my satisfaction by Dr. Gross and his staff.
- I understand my diagnosis
- I am well informed about the procedure
- I understand the material Risks and benefits of the operation.
- I know the probability of success
- I understand that the prognosis for my condition is persistent and most likely increasing pain and disability if I do not have an operation.
- I have been advised of the alternatives which include activity modification, medications such as Tylenol and anti-inflammatory medications, narcotic painkillers (not advisable), physical therapy, and various injections of steroid, PRP , Visco supplementation, and stem cells.
- I know that a stemmed total hip replacement is an alternative and is in fact the standard operation for my condition, but I believe that hip resurfacing is likely to give me a better outcome.
- I know what the likely outcome is.
- Dr. Gross is the operating surgeon (No trainee will perform your operation).
- Dr. Gross developed the Recap implants but no longer receives royalties for these implants.
- Recap/Magnum were made previously by Zimmer Biomet, they are now manufactured using the same design by Signature Orthopedics.
- Recap and Magnum components are FDA approved. Use as a total hip resurfacing is however considered off-label.
- Smith Nephew BHR components are FDA approved for use as a total hip resurfacing in men. Their use in women is considered off-label and is recommended against by the company. I disagree and use them in women.
- The Joint Medica Polymotion is available as part of an FDA IDE study with some restrictions. During the study I am bound to follow these.
- Information from your treatment is used for research purposes, but you will not be identified.
If you have any questions about the above information, please don’t hesitate to ask.

Patient to complete this section:
I (patient name:_______________________________) have reviewed the above and understand the risks and benefits involved with this operation. I would like Dr. Thomas Gross to perform hip resurfacing on me.
I also understand that all data from my case will be collected and used for research purposes mainly to continue to improve the quality of Dr. Gross’ work and to inform future patients and the world about hip resurfacing. My privacy will be protected by anonymizing the data before any publication. I agree to honor my commitment to provide timely follow up information. I agree to be contacted for follow-up due reminders via the contact info I have provided. I understand that providing this information will benefit not only me, but also Dr. Gross and many future patients of his practice and elsewhere. I hereby agree to play my part in furthering the practice and science of joint replacement surgery. At any time I can opt out of providing any further follow-up information. I do not consent for my data anonymized or otherwise to be used by attorneys not representing Dr. Gross.
Patient Signature _______________________________ Date _______________________________
Witness Signature _______________________________ Date _______________________________